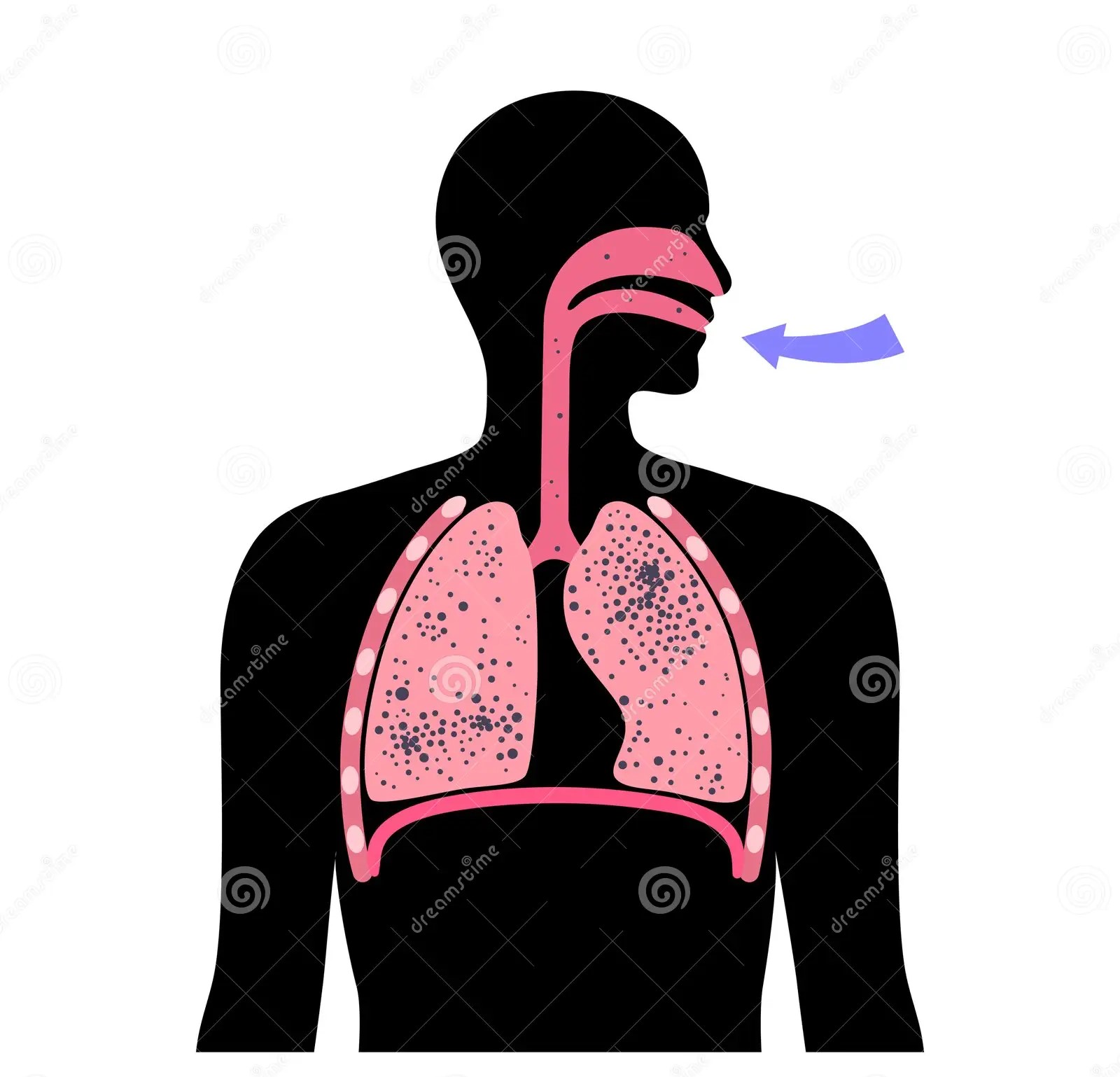
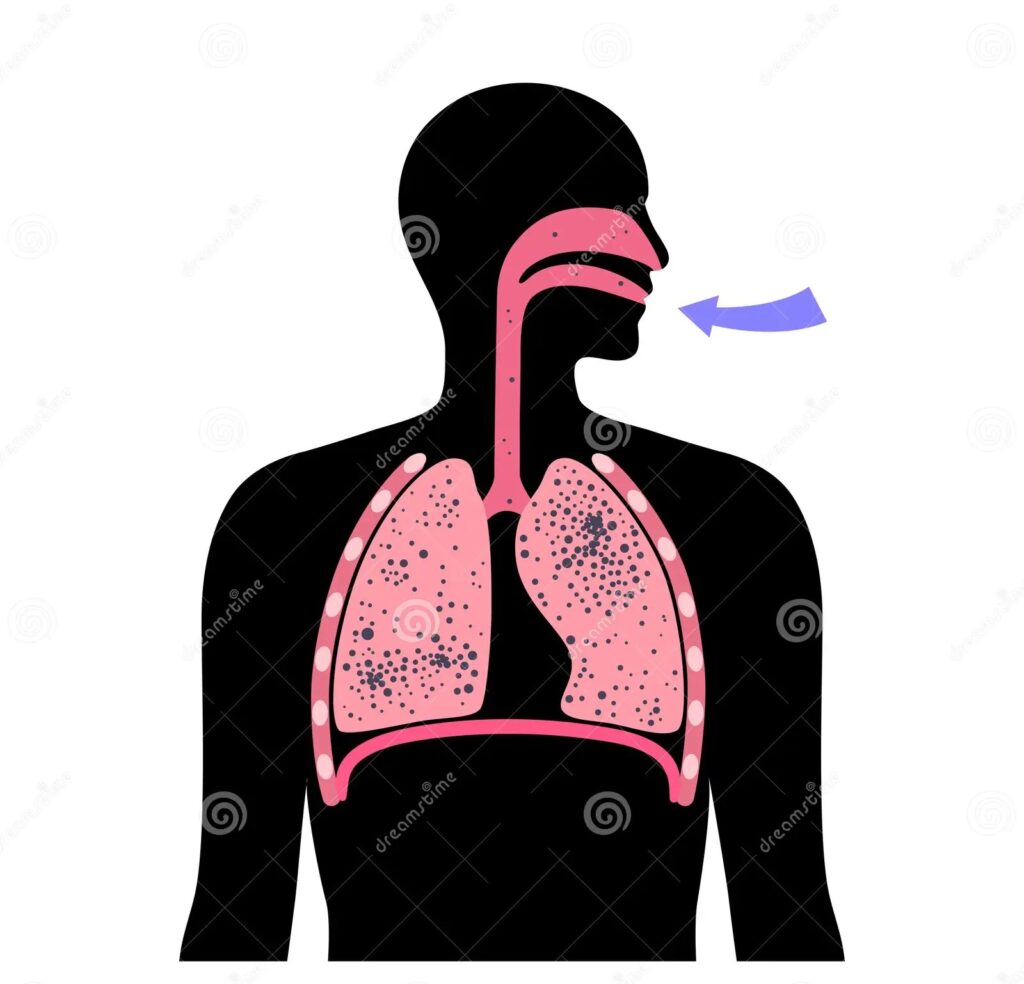
Dusts in the size range of 0.5 to 3 microns are hazardous to health and, after varying degrees of exposure, lead to a lung disease known as pneumoconiosis, which can gradually paralyse a person by reducing their ability to work due to pulmonary fibrosis and other complications. The hazardous effects of dusts on the lungs depend on a number of factors, such as (a) the chemical composition, (b) the fineness, (c) the concentration of dust in the air, (d) the duration of exposure and (e) the health status of the exposed person. In addition to the toxic effect of dust on lung tissue, the superimposition of infections such as tuberculosis can also influence the pattern of pneumoconiosis. The most important dust diseases are silicosis, anthracosis, byssinosis, bagassosis, asbestosis and farmer’s lung.
Silicosis:
Among occupational diseases, silicosis is the main cause of permanent disability and death. Inhalation of dust containing free silicon dioxide or silica causes it. It was first detected in India in 1947 in the gold mines of Kolar (Mysore). Since then, researchers have detected its presence in various other industries such as mining (coal, mica, gold, silver, lead, zinc, manganese, and other metals), ceramics, pottery, sandblasting, metal grinding, construction, rock quarrying, iron and steel, and several others.
The occurrence of silicosis depends on the chemical composition of the dust, the size of the particles, the duration of exposure and individual susceptibility. The higher the concentration of free silica in the dust, the greater the risk. Particles with a size of 0.5 to 3 microns are the most dangerous as they easily enter the lungs. The longer the exposure lasts, the greater the risk of developing silicosis. The factors mentioned above can cause the incubation period to vary from a few months to 6 years
clinical features:
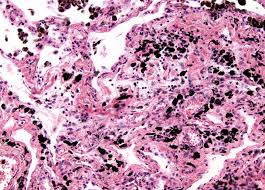
Clinically, the onset of the disease is insidious. Early symptoms include a chesty cough, shortness of breath on exertion and chest pain. The disease progresses, impairing the total lung capacity (TLC). An X-ray of the chest shows a “snowstorm” appearance in the lung fields. Silicosis is progressive, and more importantly, silicosis sufferers are susceptible to pulmonary tuberculosis, a disease known as “silicotuberculosis”
treatment:
There is no effective treatment for silicosis. “Fibrotic changes irreversibly occur once they have been initiated. The only way to contain (if not eliminate) silicosis is through (a) strict dust control measures, e.g., substitution, full enclosure, isolation, hydroblasting, good housekeeping, personal protective measures, and (b) regular physical examinations of workers.
Anthracosis:
Coal workers experience two general phases of pneumoconiosis, according to studies – (1) Simple pneumoconiosis is called the first phase, and it causes mild respiratory impairment. This phase may only develop after about 12 years of occupational exposure. (2) During the second phase, progressive massive fibrosis (PMF) causes severe respiratory impairment and often leads to premature death. Once a coal worker has simple pneumoconiosis, it can develop into progressive massive fibrosis without further exposure.
Byssinosis:

Byssinosis is due to the inhalation of cotton fibre dust over a long period of time. The symptoms are chronic cough and progressive shortness of breath, resulting in chronic bronchitis and emphysema. India has a large textile industry, which employs almost 35 of factory workers. The surveys conducted in Mumbai, Ahmedabad, and Delhi reported an incidence of bystosis ranging from 7 to 8 percent.
Bagassosis:

Workers can develop Bagassosis, a name for an occupational lung disease, by inhaling bagasse or sugar cane dust. It was first described in 1955 by Ganguli and Pal. A thermophilic actinomycete, identified as Thermoactinomyces sacchari, causes Bagassosis symptoms: shortness of breath, cough, hemoptysis, and mild fever. Initially there is acute diffuse bronchiolitis. The scigram may show spotting in the lungs or a shadow. The impairment affects lung function. With early treatment, the acute inflammation of the lungs subsides. If it remains untreated, diffuse fibrosis, emphysema and bronchiectasis develop.
PREVENTIVE MEASURES:
- DUST CONTROL: Measures for the prevention and suppression of dust such as wet process, enclosed apparatus, exhaust ventilation etc., should be used.
- PERSONAL PROTECTION: Personal protective equipment (masks or respirators with mechanical filters or with oxygen or air supply) may be necessary.
- MEDICAL CONTROL: Initial medical examination and periodical medical check-ups of the workers are indicated.
- BAGASSE CONTROL: By keeping the moisture content above 20 per cent and spraying the bagasse with 2 per cent propionic acid, a widely used fungicide, bagasse can be rendered safe for manufacturing use.
Asbestosis:
Bases such as magnesium, iron, calcium, sodium, and aluminum combine with silica to form silicates. Asbestos is of two types – serpentine or chrysolite variety and the amphibole type. Asbestos fibres are usually from 20 to 500 μ in length and 0.5 to 50 μ in diameter. In the manufacture of asbestos cement, fire-proof textiles, roof tiling, brake lining, gaskets, and several other items, asbestos is employed.
The body takes in the fine dust by inhaling, and it gets deposited in the alveoli. The fibres are insoluble. The dust deposited in the lungs causes pulmonary fibrosis leading to respiratory insufficiency and death; carcinoma of the bronchus; mesothelioma of the pleura or peritoneum; and cancer of the gastro-intestinal tract. Mesothelioma, a rare form of cancer affecting the pleura and peritoneum, is strongly associated with the use of crocidolite asbestos. The fibrosis in asbestosis is due to mechanical irritation, and is peri-bronchial, diffuse in character.
clinical features:
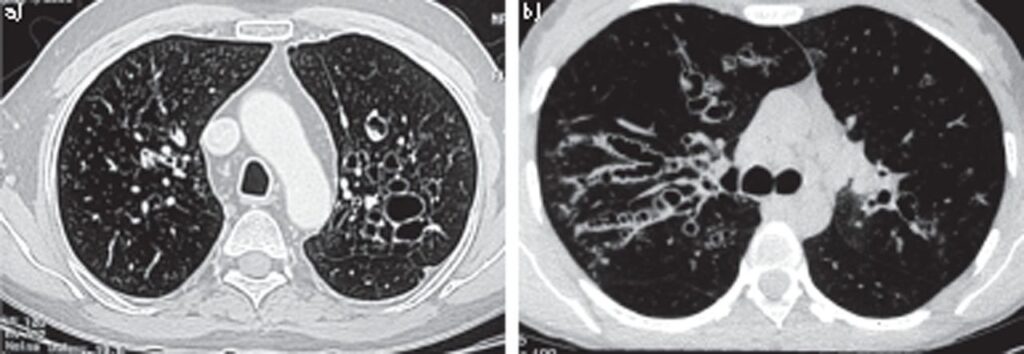
Clinically the disease is characterized by dyspnoea which is frequently out of proportion to the clinical signs in the lungs. In advanced cases, there may be dubbing of fingers, cardiac distress and cyanosis. Asbestos fibres coated with fibrin are found in the sputum as asbestos bodies. An X-ray of the chest shows a ground-glass appearance in the lower two thirds of the lung fields.
preventive measures:
- use of safer types of asbestos (chrysolite and amosite)
- substitution of other insulants: glass fibre, mineral wool, calcium silicate, plastic foams
- rigorous dust control
- periodic examination of workers; biological monitoring (clinical, X-ray, lung function)
- continuing research
Farmer’s lung:
Farmer’s lung is due to the inhalation of mouldy hay and grain dust. In grain dust or hay with a moisture content of over 30 per cent bacteria and fungi grow rapidly, causing a rise of temperature to 40 to 50 deg. C. This heat encourages the growth of thermophilic actinomycetes, of which Micropolyspora faeni is the main cause of farmer’s lung. The acute illness is characterized by general and, respiratory symptoms and physical signs. Repeated attacks, cause pulmonary fibrosis and inevitable pulmonary damage and corpulmonale.
 Users Today : 2
Users Today : 2 Users Yesterday : 3
Users Yesterday : 3 Users Last 7 days : 18
Users Last 7 days : 18 Users Last 30 days : 103
Users Last 30 days : 103 Users This Month : 74
Users This Month : 74