Hypertension is a chronic condition of concern due to its role in the causation of coronary heart disease, stroke and other vascular complications. It is the commonest cardiovascular disorder, posing a major public . health challenge to population in socio-economic and epidemiological transition. Raise blood pressure is one of the major risk factors for cardiovascular mortality, which accounts for 20-50 percent of all deaths.
Classification of blood pressure measurements :
| Category | Systolic blood pressure (mmHg) | Diastolic blood pressure (mmHg) |
| Normal | < 120 | <80 |
| Pre-hypertension | 120-139 | 80-90 |
| Hypertension | ||
| Stage 1 | 140-159 | 90-99 |
| Stage 2 | >160 | >100 |
secondary. Hypertension is classified as “essential” when the causes are generally unknown. Essential hypertension is the most prevalent form of hypertension accounting for 90 percent of all cases of hypertension. Hypertension is classified as “secondary” when some other disease process or abnormality is involved in its causation.
Blood pressure measurement :
Despite more than 75 years of experience with the measurement of blood pressure, discussion continues about its reliability and wide variability in individual subjects. Accurate measurements are essential under standardized conditions for valid comparison between persons or groups over time.
Three sources of errors have been identified in the recording of blood pressure : (a) Observer errors: e.g., hearing acuity, interpretation of Korotkow sounds. (b) Instrumental errors : e.g., leaking valve, cuffs that.do not encircle the arm. If the cuff is too small and fails to encircle the arm properly then too high a reading will be obtained; and (c) Subject errors : e.g., the circumstances of examination. These include the physical environment, the position of the subject, external stimuli such as fear, anxiety, and so on.
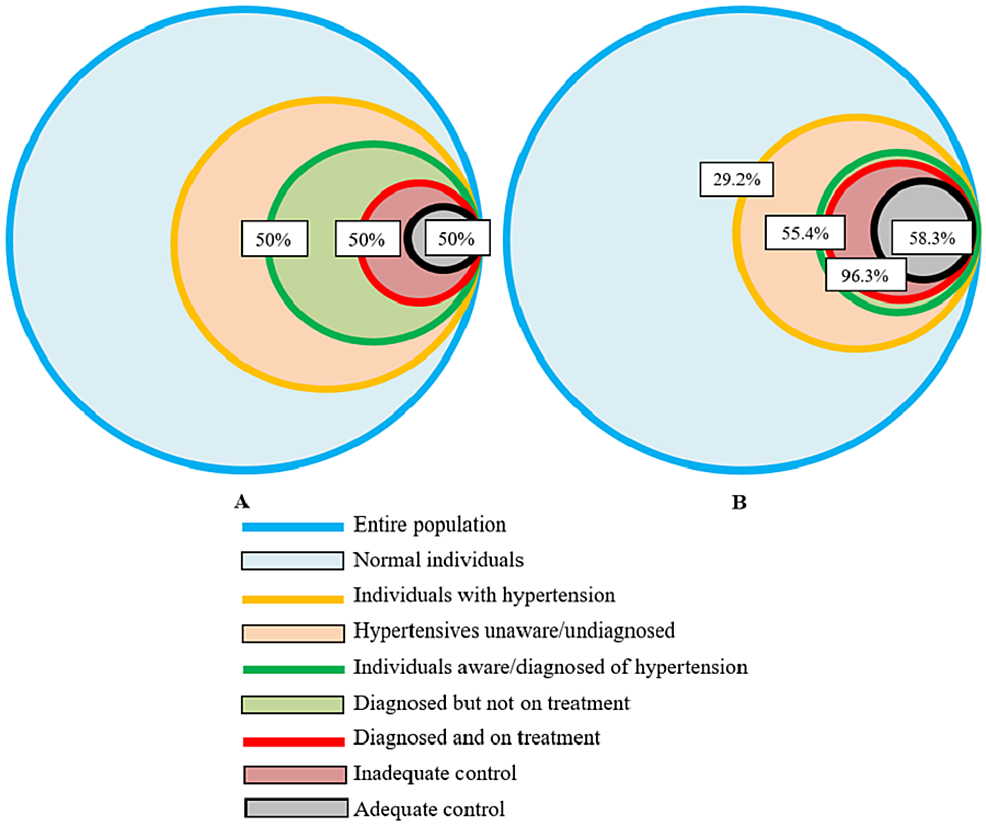
“Rule of halves” :
Hypertension is an “iceberg” disease. It became evident in the early 1970s that only about half of the hypertensive subjects in the general population of most developed countries were aware of the condition, only about half of those aware of the problem were being treated, and only about half of those treated were considered adequately treated. If this was the situation in countries with highly developed medical services, in the developing countries, the proportion treated would be far too less.
Risk factors for hypertension :
Hypertension is not only one of the major risk factors for most forms of cardiovascular disease, but that it is a
condition with its own risk factors. A WHO Scientific Group has recently reviewed the risk. factors for essential
hypertension. These may be classified as :
Non-modifiable risk factors :
(a) AGE :
Blood pressure rises with age in both sexes and the rise is greater in those with higher initial blood pressure. Age probably represents an accumulation of environmental influences and the effects of genetically programmed senescence in body systems.
(b) SEX:
Early in life there is little evidence of a difference in blood pressure between the sexes. However, at adolescence, men display a higher average level. Post-menopausal changes in women may be
the contributory factor for this change. Studies are in progress to evaluate whether oestrogen.
(c) GENETIC FACTORS:
There is considerable evidence that blood pressure levels are determined in part by genetic
factors, and that the inheritance is polygenic. The evidence is based on twin and family studies. Twin studies have confirmed the importance of genetic factors in hypertension.
(d) ETHNICITY :
Population studies have consistently revealed higher blood pressure levels in black communities
than other ethnic groups. Average difference in blood pressure between the two groups vary from slightly less than 5 mm Hg during the second decade of life to nearly 20 mm Hg during the sixth.
Modifiable risk factors :
(a) OBESITY :
Epidemiological observations have identified obesity as a risk factor for hypertension. The greater the weight gain, the greater the risk of high blood pressure. Data also indicate that when people with high blood pressure lose weight, their blood pressure generally decreases.
(b) SALT INTAKE :
There is an increasing body of evidence to the effect that a high salt intake (i.e., 7-8 g per day) increases blood pressure proportionately. Low sodium, intake has been found to lower the blood pressure. For
instance, the higher incidence of hypertension is found in Japan where sodium intake is above 400 mmol/day while primitive societies ingesting less than 60 mmol/day have virtually no hypertension (16). It has been postulated that essential hypertensives have a genetic abnormality of the kidney which makes salt excretion difficult except at raised levels of arterial pressure.
(c) SATURATED FAT :
The evidences suggest that saturated fat raises blood pressure as well as serum cholesterol.
(d) DIETARY FIBRE :
Several studies indicate that the risk of CHD and hypertension is inversely related to the
consumption of dietary fibre. Most fibres reduce plasma total and LDL cholesterol
(e) ALCOHOL:
High alcohol intake is associated with an increased risk of high blood pressure. It appears that alcohol consumption raises systolic pressure more than the diastolic.
(f) HEART RATE :
When groups of normotensive and untreated hypertensive subjects, matched for age and sex, are compared, the heart rate of the hypertensive group is invariably higher. This may reflect a resetting of sympathetic activity at a higher level. The role of heart variability in blood pressure needs further research to elucidate whether the relation is casual or prognostic.
(g) PHYSICAL ACTIVITY:
Physical activity by reducing body weight may have an indirect effect on blood pressure.
(h) ENVIRONMENTAL STRESS :
The term hypertension itself implies a disorder initiated by tension or stress. Since stress is nowhere defined, the hypothesis is untestable. Virtually all studies on blood pressure and catecholamine levels in young people revealed significantly higher noradrenaline levels in hypertensives than in normotensives.
(i) SOCIO-ECONOMIC STATUS :
In countries that are in post-transitional stage of economic and epidemiological change, consistently higher levels of blood pressure have been noted in lower socio-economic groups.
(j) OTHER FACTORS :
The commonest present cause of secondary hypertension is oral contraception, because of the oestrogen component in combined preparations. Other factors such as noise, vibration, temperature and humidity
require further investigation.
 Users Today : 1
Users Today : 1 Users Yesterday : 2
Users Yesterday : 2 Users Last 7 days : 16
Users Last 7 days : 16 Users Last 30 days : 102
Users Last 30 days : 102 Users This Month : 75
Users This Month : 75